Many people think IBS and IBD are the same thing. Both cause belly pain, diarrhea, and bloating. But they’re not just similar-they’re fundamentally different. One is a functional disorder. The other is a structural disease. Mixing them up can lead to the wrong treatment, delayed care, or unnecessary worry. Here’s what actually separates them.
What Is IBS?
IBS, or Irritable Bowel Syndrome, is a functional disorder. That means your gut looks normal on scans and biopsies-but it doesn’t work right. There’s no inflammation, no ulcers, no damage. Your nerves and muscles just react differently to food, stress, or gas.
The Rome IV criteria, used by doctors worldwide since 2016, define IBS by three key things: abdominal pain at least once a week for three months, plus two of these: pain linked to bowel movements, change in stool frequency, or change in stool form. You might have diarrhea most days, or constipation, or switch between both. Bloating is common-76% of people with IBS report it. Mucus in stool? That happens in about 45% of cases. But here’s the catch: no blood.
Doctors rule out IBD before diagnosing IBS. That means normal blood tests, negative stool tests for infection or inflammation, and a clean colonoscopy. If you’ve had a colonoscopy and the doctor said your lining looked perfect? That’s a good sign you’re dealing with IBS, not IBD.
IBS doesn’t get worse over time. It doesn’t cause cancer. It doesn’t lead to surgery. It doesn’t shorten your life. But it can wreck your quality of life. A 2016 study from Beth Israel Deaconess Medical Center found people with IBS would give up caffeine, their phone, even sex to be free of symptoms. That’s how disruptive it can be.
What Is IBD?
IBD stands for Inflammatory Bowel Disease. It’s not one condition-it’s two: Crohn’s disease and ulcerative colitis. Both involve chronic, visible inflammation that damages the gut lining. Unlike IBS, this damage shows up on scans, biopsies, and even in blood tests.
In ulcerative colitis, inflammation is limited to the colon and rectum. It causes ulcers that bleed-92% of patients have bloody stools at diagnosis. In Crohn’s disease, inflammation can hit anywhere from mouth to anus. It creates deep sores, strictures (narrowing), and fistulas (abnormal tunnels). About 33% of Crohn’s patients develop strictures within 10 years. Around 17% get fistulas.
IBD doesn’t just affect the gut. It can cause joint pain, eye inflammation (uveitis), skin rashes like erythema nodosum, and liver issues. These are called extraintestinal symptoms-and they’re rare in IBS. If you have joint swelling or red, painful bumps on your shins? That’s more likely IBD.
Lab tests show clear signs. Fecal calprotectin, a marker of gut inflammation, is usually above 250 µg/g in active IBD. Normal is under 50. CRP, a blood marker for inflammation, is often above 5 mg/L in IBD-normal is under 3. These numbers don’t budge in IBS. They stay flat.
The Big Difference: Damage vs. Dysfunction
The easiest way to tell them apart? Look for physical damage.
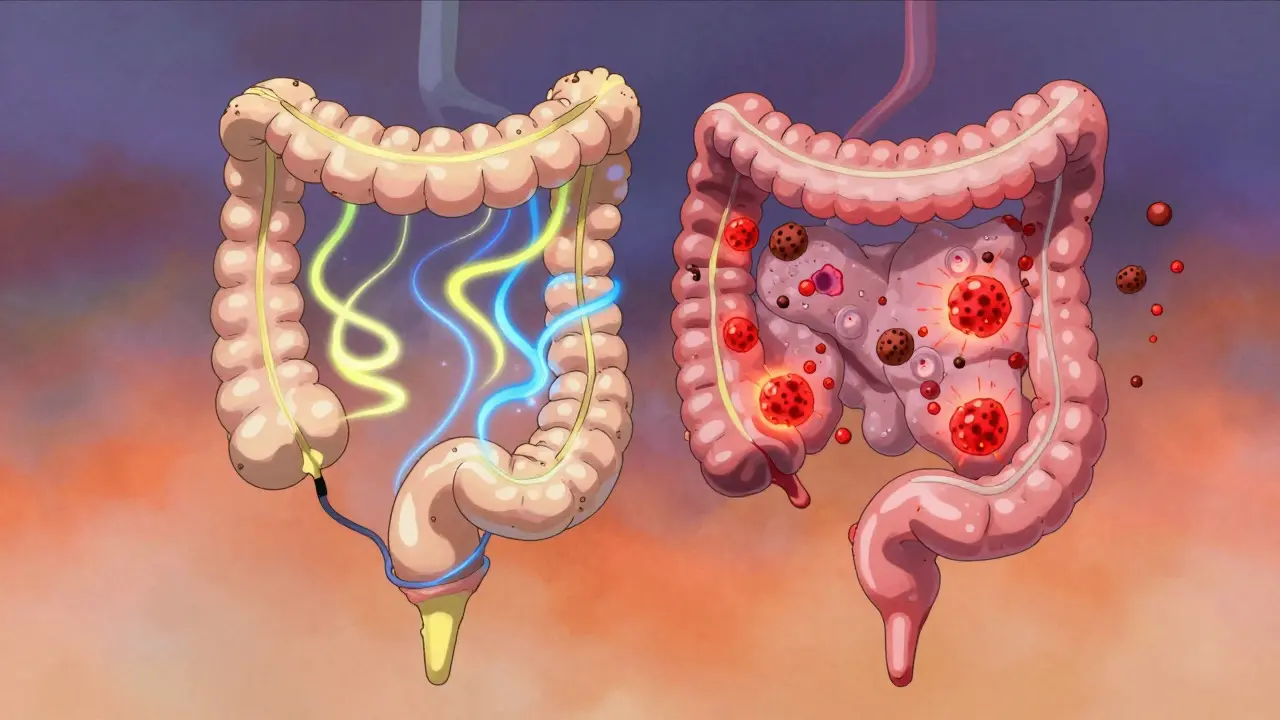
IBS: no structural change. Your colon looks fine. Tests come back normal. You feel awful, but your body isn’t breaking down.
IBD: inflammation is tearing at your gut. Biopsies show immune cells attacking tissue. Scans reveal ulcers, thickened walls, or narrowed passages. Blood tests scream inflammation.
This isn’t semantics. It’s life-changing. If you have IBD and aren’t treated, you risk serious complications: colorectal cancer (2% risk per year after 10 years of pancolitis), toxic megacolon (a life-threatening dilation of the colon), or bowel perforation. IBS doesn’t do any of this.
Dr. Baidoo from Regional One Health puts it plainly: "IBD is a structural disease. Symptoms come from physical damage. IBS is functional. No damage. Just misfiring signals."
How Are They Diagnosed?
IBS is diagnosed by excluding everything else. If your symptoms match the Rome IV criteria, and your colonoscopy, blood tests, and stool tests show no inflammation or infection? You likely have IBS.
IBD is diagnosed by finding damage. Colonoscopy with biopsy is the gold standard. In 98% of confirmed cases, pathologists see inflamed tissue, crypt abscesses, or granulomas (clumps of immune cells). MRI enterography finds Crohn’s complications with 92% accuracy. Blood tests show elevated CRP and calprotectin. Stool tests rule out infections like C. diff.
Alarm signs? If you have any of these, skip the IBS label and see a doctor right away:
- Bloody stool
- Unexplained weight loss
- Fever without infection
- Anemia (low iron)
- Family history of colon cancer or IBD
These are red flags for IBD. They’re not part of IBS.
How Are They Treated?
IBS treatment is about managing symptoms-not curing inflammation, because there isn’t any.
Low-FODMAP diet? It works for 76% of people. That’s a big deal. It reduces gas, bloating, and pain by cutting out hard-to-digest carbs. Probiotics, peppermint oil, and fiber supplements help some. For pain and diarrhea, low-dose antidepressants (like amitriptyline) can calm nerve signals. Eluxadoline helps IBS-D patients by slowing gut movement. It’s not a miracle, but it helps 35-40% of users.
IBD treatment is about stopping inflammation before it destroys your gut.
First line: corticosteroids. They work fast-70-80% of flares improve. But they’re not for long-term use. Side effects pile up: weight gain, bone loss, diabetes.
Second line: biologics. Drugs like infliximab (Remicade) and vedolizumab (Entyvio) block specific parts of the immune system. Infliximab puts 50-60% of Crohn’s patients into remission within 14 weeks. Vedolizumab helps 48% of ulcerative colitis patients stay in remission after a year.
Some people need surgery. Up to 70% of ulcerative colitis patients eventually have their colon removed. Crohn’s patients may need bowel resections. These aren’t failures-they’re necessary to stop damage.

Can You Have Both?
Yes. And it’s more common than you think.
Studies show 22-35% of people with IBD in remission still meet the Rome IV criteria for IBS. Their inflammation is under control, but their gut still acts up-cramps, bloating, urgency. That’s not a flare. That’s IBS on top of IBD.
Doctors now recognize this. If you have IBD and your inflammation markers are normal but you still have symptoms, they’ll check for IBS too. You don’t have to choose one or the other. You can have both.
Myth Busting
- Myth: IBS turns into IBD. Truth: It never does. The Crohn’s & Colitis Foundation says this outright: "IBS does not develop into IBD."
- Myth: Stress causes IBD. Truth: Stress doesn’t cause it, but it can trigger flares. IBS, on the other hand, is heavily tied to stress and anxiety.
- Myth: IBD is just "bad IBS." Truth: No. IBD is an autoimmune disease. IBS isn’t. They’re on different sides of the medical spectrum.
One thing both share? They’re invisible. No one can see your pain. But that doesn’t make it less real. Both conditions are debilitating. Both need understanding. But only one needs urgent medical intervention.

















